

The right lung has three lobes whereas the left has two lobes and a lingula. Each lung is enclosed by parietal pleura. The parietal pleura are innervated by somatic sensory nerves, which allow the sensation of sharp and localized pain.
The lungs are attached to the trachea and the heart. The pulmonary circulation supplies the respiratory tissues with deoxygenated blood, whereas the bronchial vessels nourish the nonrespiratory tissues with oxygenated blood.
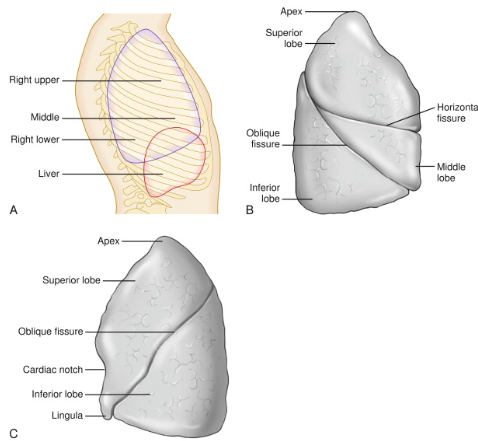
A, Lobes of the lung. B, Detailed anatomy of the right lung, demonstrating the horizontal fissure (separating the superior from middle lobe) and the oblique fissure (separating the middle from inferior lobe). C, More detailed anatomy of the left lung, demonstrating the lingula at the base of the superior lobe.
Parasympathetic innervation to the lung causes bronchoconstriction, whereas sympathetic innervation causes with oxygenated blood.
Trachea and Bronchi
The trachea courses from the larynx into the thorax, where the trachea bifurcates at the carina into the right and left primary mainstem bronchi at the T4–T5 vertebral level.
The right main bronchus is wider, shorter and more vertical than the left main bronchus. Consequently, aspirated foreign bodies are far more likely to enter and obstruct the bronchi of the right side of the lung. An object aspirated while standing or sitting upright will usually be found in the inferior portion of the right lower lobe whereas an object aspirated while supine will most often end up in the superior portion of the right lower lobe
The right primary bronchus divides into superior, middle, and inferior secondary (lobar) bronchi, corresponding to superior, middle, and inferior lobes of the right lung, respectively. The left primary bronchus divides into superior and inferior secondary bronchi, corresponding to superior and inferior lobes of the left lung, respectively.
Bronchopulmonary
Each secondary bronchus further divides into tertiary (segmental) bronchi, which further divide. The smallest bronchi give rise to bronchioles, which terminate in alveolar sacs where the exchange of gases occurs.

A. Right lung in medial view. B. Bronchial tree and lungs. C. Left lung in medial view.
The trachea bifurcates into the left and right main bronchi at the carina. For the USMLE Step 1, it is important to know that the right main bronchus is wider, shorter and more vertical than the left main bronchus. Consequently, aspirated foreign bodies are far more likely to enter and obstruct the bronchi of the right side of the lung. An object aspirated while standing or sitting upright will usually be found in the inferior portion of the right lower lobe whereas an object aspirated while supine will most often end up in the superior portion of the right lower lobe (See Figure Below). ). (usmle emphasis)

Bronchopulmonary Segments
Each
bronchopulmonary segment
of the lung has its own neurovascular supply that is not shared with surrounding bronchopulmonary segments (see
Fig. 17-2
). This is important because each bronchopulmonary segment can function independently; a single segment can be removed surgically (e.g., to remove a tumor) without affecting the other segments. The trachea bifurcates into the right and left main bronchi at the carina. These main bronchi divide further into lobar bronchi, which subsequently divide into segmental bronchi, totaling 10 in each lung. A single segmental bronchus is the core of each bronchopulmonary segment. In addition to a segmental bronchus, each bronchopulmonary segment is also composed of the following:
This is important because each bronchopulmonary segment can function independently; a single segment can be removed surgically (e.g., to remove a tumor) without affecting the other segments. The trachea bifurcates into the right and left main bronchi at the carina. These main bronchi divide further into lobar bronchi, which subsequently divide into segmental bronchi, totaling 10 in each lung. A single segmental bronchus is the core of each bronchopulmonary segment. In addition to a segmental bronchus, each bronchopulmonary segment is also composed of the following:
❍ One branch of the pulmonary artery. These branches carry deoxygenated blood from the right side of the heart and are centrally located within the bronchopulmonary segment.
❍ Pulmonary veins that return oxygenated blood that has undergone gas exchange to the left atrium. These are located peripherally within each segment.
❍ One branch of the bronchial artery . These branches originate from the thoracic aorta and carry highly oxygenated blood to supply the lung parenchyma and stroma. Like the pulmonary artery branch, the bronchial artery is also centrally located within each segment.
The lungs are supplied with a dual circulation. The pulmonary arteries arise from the right ventricle to supply the pulmonary parenchyma in a low-pressure circuit. The bronchial arteries arise from the aorta or intercostal arteries and carry blood under systemic pressure to the airways, blood vessels, hila, and visceral pleura. Although the bronchial circulation represents only 1–2% of total pulmonary blood flow, it can increase dramatically under conditions of chronic inflammation—eg, chronic bronchiectasis—and is frequently the source of hemoptysis.
❍ Bronchial veins, located peripherally along each segment, which return deoxygenated blood that has circulated through the lung parenchyma and stroma to the azygous venous system.
❍ Lymphatics, located peripherally along each segment.
❍ Autonomic fibers , located around the segmental bronchi and blood vessels. These are comprised of parasympathetic branches from the vagus nerve, which innervate smooth muscle in the walls of terminal bronchioles, and sympathetic fibers, which innervate vascular smooth muscle.
Regions of the Lung
Each lung has the following regions corresponding to its respective regions of the chest:
- Costal lung surface. The large convex area related to the inner surface of the ribs.
- Mediastinal lung surface. The medial concave surface containing the root (hilum) of the lungs related to the heart. This surface contains a mainstem bronchus and a pulmonary artery and pulmonary veins, nerves, and lymphatics.
- Diaphragmatic lung surface. The base of the lungs, which are convex because they rest on the domed diaphragm.
- Apex of the lung. This area projects into the root of the neck and is crossed anteriorly by the subclavian artery and vein.
Lobes of the Lung
Each lung is divided into lobes with its own covering of visceral pleura.
- The right lung has three lobes (superior, middle, and inferior), which are divided by a horizontal and an oblique fissure (Figure 3-2A). The right lung is shorter and wider than the left because of the higher right dome of the diaphragm and because the heart bulges more into the left side of the thorax.
- The left lung has only two lobes (superior and inferior), which are divided by an oblique fissure along the sixth rib. Instead of having a middle lobe, the left lung has a space occupied by the heart. Therefore, the left lung has a cardiac notch as well as the lingula, an extension of the left superior lobe into the left costomediastinal recess.
Each lung is located in its respective pleural cavity enclosed by parietal pleura. The parietal pleura are innervated by somatic sensory nerves, which allow the sensation of sharp and localized pain. Inflammation of the pleura causes pain that worsens on inspiration and is referred to as pleuritic chest pain. This characteristic pain can help distinguish pulmonary pathology (e.g., pneumonia, pneumothorax, pulmonary embolism) from cardiac pathology (e.g., myocardial infarction).

One can remember the relationship of pulmonary artery to the main bronchus at each lung hilus by RALS—R ight A nterior L eft S uperior.
Vasculature of the Lung
The pulmonary and bronchial arteries and veins provide dual vascular supply. These two supplies can be confusing. In a nutshell, here is the information you need to know about the vascular supply: Pulmonary arteries and veins deal with gas exchange and the circulation of blood between the heart and lungs, whereas the bronchial arteries and veins are the vascular supply to the structural elements of the lungs, such as the bronchial tree.
- Pulmonary arteries. Branch from the pulmonary trunk, which receives blood from the right ventricle of the heart (Figure 3-3A). Pulmonary arteries deliver deoxygenated blood from the systemic circulation to exchange carbon dioxide with oxygen in the lungs. At the bifurcation of the pulmonary trunk into the pulmonary arteries, there is a connection to the aortic arch via the ligamentum arteriosum, the fibrous remnant of the fetal ductus arteriosus. One can remember the relationship of pulmonary artery to the main bronchus at each lung hilus by RALS—R ight Anterior L eft S uperior.
- Pulmonary veins. Transport oxygenated blood from the pulmonary capillaries to the left atrium of the heart. They do not accompany the bronchi or the segmental arteries within the lung parenchyma. Two pulmonary veins exit the left lung and three pulmonary veins exit the right lung (one for each lobe), but the right upper and middle veins usually join so that usually only four pulmonary veins enter the left atrium.
- Bronchial arteries. Branch from the thoracic (descending) aorta and supply the bronchial tree. There is usually one bronchial artery for the right lung and two for the left lung.
- Bronchial veins. Drain the bronchi. The bronchial veins receive blood from the larger subdivisions of the bronchi and empty into the azygos vein on the right and the accessory hemiazygos vein on the left. Some bronchial veins become tributaries to the pulmonary veins.
At total lung capacity, the lung fills the entire chest cavity and can reach a volume, in the adult human, of some 5 to 6 L, largely depending on body size. Upon expiration, the lung retracts, most conspicuously from the lower parts of the pleural cavity, the posterior bottom edge of the lung moving upward by some 4 to 6 cm. This preferential lifting of the bottom edge is caused by retraction of the tissue throughout the entire lung, the surfaces of which are freely movable within the thoracic cavity.
The pulmonary circulation i carries deoxygenated blood away from the right ventricle to the lungs, and returns oxygenated (oxygen-rich) blood to the left atrium heart.
A separate system, the bronchial circulation, supplies blood to the tissue of the larger airways of the lung.
Pulmonary arteries and veins deal with gas exchange and the circulation of blood between the heart and lungs,
whereas the bronchial arteries and veins are the vascular supply to the structural elements of the lungs, such as the bronchial tree.
- Pulmonary arteries. Branch from the pulmonary trunk, which receives blood from the right ventricle of the heart (Figure 3-3A). Pulmonary arteries deliver deoxygenated blood from the systemic circulation to exchange carbon dioxide with oxygen in the lungs. At the bifurcation of the pulmonary trunk into the pulmonary arteries, there is a connection to the aortic arch via the ligamentum arteriosum, the fibrous remnant of the fetal ductus arteriosus. One can remember the relationship of pulmonary artery to the main bronchus at each lung hilus by RALS—R ight A nterior L eft S uperior.
- Pulmonary veins. Transport oxygenated blood from the pulmonary capillaries to the left atrium of the heart. They do not accompany the bronchi or the segmental arteries within the lung parenchyma. Two pulmonary veins exit the left lung and three pulmonary veins exit the right lung (one for each lobe), but the right upper and middle veins usually join so that usually only four pulmonary veins enter the left atrium.
- Bronchial arteries. Branch from the thoracic (descending) aorta and supply the bronchial tree. There is usually one bronchial artery for the right lung and two for the left lung.
- Bronchial veins. Drain the bronchi. The bronchial veins receive blood from the larger subdivisions of the bronchi and empty into the azygos vein on the right and the accessory hemiazygos vein on the left. Some bronchial veins become tributaries to the pulmonary veins.
-

A. Pulmonary plexus. B. Autonomic innervation of the lung.
Lymphatics of the Lung
Lymph from lobes of the lungs drains into pulmonary and bronchopulmonary (hilar) nodes and then into the tracheobronchial (carinal) nodes and into the paratracheal nodes en route to drain into either the right lymphatic duct (for the right lung) or the thoracic duct (for the left lung). It should be noted that no lymphatics are present in the walls of the alveolar sacs.
The pulmonary plexus follows the trachea and bronchial tree, providing parasympathetic and sympathetic innervation to the smooth muscle and glands of the lungs (Figure 3-3B). The pulmonary plexus is divided and named according to its position to the root of the lung, where the anterior pulmonary plexus lies anterior and the posterior pulmonary plexus lies posterior to the corresponding bronchus. Branches of the pulmonary plexus accompany the blood vessels and bronchi into the lung as well.
- Parasympathetic innervation. The pulmonary plexus receives preganglionic parasympathetic and visceral sensory innervation via the vagus nerves. The vagus nerves are the tenth pair of cranial nerves and have the widest field of distribution to the body. They innervate structures in the head, neck, thorax, and abdomen. In the thorax, the vagus nerves provide all the parasympathetic innervation of the viscera. Parasympathetic innervation causes bronchoconstriction of the smooth muscle of the bronchial tree, vasodilation of the pulmonary vessels, and secretion from bronchial glands.
- Sympathetic innervation. Postganglionic sympathetic fibers from the T1 to T4 levels of the sympathetic trunk and cervical sympathetic ganglia contribute to the pulmonary plexus. Sympathetic innervation causes bronchodilation, vasoconstriction of the pulmonary vessels, and inhibition of secretion from the bronchial glands. Visceral sensory fibers from the visceral pleura and bronchi may also accompany sympathetic fibers.
A bronchopulmonary segment consists of a lobar (segmental or tertiary) bronchus, a corresponding branch of the pulmonary artery, and the supplied segment of the lung tissue, all surrounded by a connective tissue septum. A bronchopulmonary segment refers to the portion of the lung supplied by each segmental bronchus and segmental artery. The pulmonary veins lie between bronchopulmonary segments.
 Surgical removal of lung segments. Bronchopulmonary segments are clinically important because they serve as the anatomic, functional, and “surgical” unit of the lungs. A surgeon may remove a bronchopulmonary segment of the lung without disrupting the surrounding lung parenchyma.
Surgical removal of lung segments. Bronchopulmonary segments are clinically important because they serve as the anatomic, functional, and “surgical” unit of the lungs. A surgeon may remove a bronchopulmonary segment of the lung without disrupting the surrounding lung parenchyma.
Content 5
Content 6
At the end of a deep breath, about 80% of the lung volume is air, 10% is blood, and only the remaining 10% is tissue. Respiration is the vital exchange of oxygen and carbon dioxide as blood circulates through the lungs. The thoracic skeleton, thoracic wall muscles, bronchial tree, and pulmonary circulation all aid in this process. Breathing is a mechanical process resulting from volume changes in the thoracic cavity with inverse changes in pleural pressure. Pressure changes lead to gas flow.
At total lung capacity, the lung fills the entire chest cavity and can reach a volume, in the adult human, of some 5 to 6 L.
Inspiration
The process of inspiration (inhalation) is easily understood if you visualize the thoracic cavity as a closed box with a single opening at the top called the trachea. The trachea allows air to move in and out of the thoracic cavity (“the box”). The volume of the thoracic cavity is changeable and can be increased by enlarging all its diameters (superior to inferior, anterior to posterior, and medial to lateral), thereby decreasing the pressure in the pleural space (pleural pressure) (Figure 3-4A and B). This, in turn, causes air to rush from the atmosphere (positive pressure relative to the lungs) into the lungs (negative pressure relative to the atmosphere) because gas flows down its pressure gradient. The muscles that primarily expand the thoracic cavity during inspiration are the diaphragm and the intercostal muscles.
- Diaphragm. In the relaxed state, the diaphragm is dome shaped. When the diaphragm contracts, it flattens, increasing the vertical dimensions and thus the volume of the thoracic cavity.
- Intercostal muscles. Contraction of the external intercostal muscles lifts the rib cage and pulls the sternum anteriorly. Because the ribs curve downward as well as forward around the chest wall, the broadest lateral and anteroposterior dimensions of the rib cage are normally directed downward. However, when the ribs are raised and drawn together, they also swing outward, expanding the diameter of the thorax both laterally and in the anteroposterior plane. This is similar to the action that occurs when a curved bucket handle is raised away from the bucket (Figure 3-4C).

Movements of the thoracic wall during inhalation and exhalation in the anterior (A) and axial superior (B) views. C. Thoracic wall movements during respiration. The bucket and water-pump handle are analogies for the movement of the rib cage when acted upon by respiratory muscles.
Although these actions expand the thoracic dimensions by only a few millimeters along each plane, this expansion is sufficient to increase the volume of the thoracic cavity by approximately 0.5 L, the approximate volume of air that enters the lungs during normal inhalation. The diaphragm is by far the most important structure that brings about the pressure, gas flow, and volume changes that lead to normal inhalation.
As the thoracic dimensions increase during inspiration, pleural pressure becomes more negative and “pulls” on the lungs as thoracic volume increases. The consequence is that the lungs expand (fill with gas) and intrapulmonary volume increases. Inspiration ends when thoracic volume ceases to increase, resulting in no further reduction in pleural pressure. Gas flow ceases and thus lung volume does not change.
During the deep or forced inspirations that occur during vigorous exercise, the volume of the thoracic cavity is further increased by activation of the accessory muscles. Accessory respiratory muscles, including the scalenes, sternocleidomastoid, and pectoralis minor, elevate the ribs more than occurs during quiet inspiration.
Expiration
Quiet expiration (exhalation) is largely a passive process that depends more on the natural elasticity of the thoracic wall and lungs than on muscle contraction. In contrast, forced expiration is an active process (Figure 3-4A–C).
- Quiet expiration. As the inspiratory muscles relax, the diaphragm ascends, the rib cage descends, and the stretched elastic tissue of the lungs recoils. Thus, both thoracic and lung volumes decrease. Decreased lung volume compresses the alveoli, resulting in increases above atmospheric pressure, thereby forcing gas flow out of the lungs. For example, when the diaphragm relaxes, it passively moves superiorly. Consequently, the vertical dimension of the thorax is decreased and thus the volume of the thoracic cavity decreases.
- Forced expiration. When the expiratory muscles (e.g., the external and internal oblique and transverse and rectus abdominis) contract, they increase intra-abdominal pressure. This forces the abdominal organs superiorly against the diaphragm, raising it. The same muscles depress the rib cage. Both actions forcibly reduce the volume in the thoracic cavity, increasing pleural volume and thence pressure in the lungs, forcing air to move from the lungs and out of the trachea.
- Upon expiration, the lung retracts, most conspicuously from the lower parts of the pleural cavity, the posterior bottom edge of the lung moving upward by some 4 to 6 cm. This preferential lifting of the bottom edge is caused by retraction of the tissue throughout the entire lung, the surfaces of which are freely movable within the thoracic cavity.
In a healthy person, blood from the pulmonary trunk will flow next into which of the following structures?
Reference: Lungs#pulmonary trunk
Content 2
Content 3